Call us


|
Added
Nov 29, 2019
Location
Views
897
Rating
  |
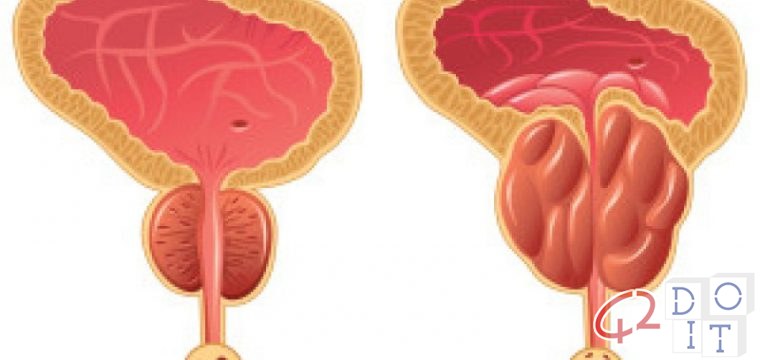
Benign prostatic hyperplasia, commonly known as an enlarged prostate, consists of an increase in the volume of the gland located immediately below the bladder. The prostate has the function of producing a part of the seminal fluid. Benign prostatic hyperplasia usually occurs after the age of 50 and is very common in the age group between 60 and 80: it is estimated to be present in half of the over 50s and in three quarters of the over-80s. 40% of patients with benign prostatic hypertrophy need treatment.
What are the causes of this enlargement?
Unfortunately the causes are still unknown. Given the concomitance of prostatic hyperplasia with advancing age, we are studying the hypothesis that the change in hormonal balance (andropause) and in particular the level of testosterone, the male hormone par excellence, can play a role in meaning that the new hormonal structure, with the variation of the androgen / estrogen ratio could favor the enlargement of the prostate gland.
What symptoms characterize benign prostatic hypertrophy?
Benign prostatic hypertrophy does not show its own symptoms but manifests itself with symptoms related to the difficulty in urinating: the enlarged gland, in fact, compress the part of the canal that connects the bladder with the outside) which crosses it narrowing the caliber and obliges the bladder to overwork to expel the accumulated urine.
Over time, this disorder can weaken and render the bladder less performing, which can become more easily infected, produce stones and make complete bladder drainage difficult until acute retention.
The symptoms that can derive from an important prostatic hyperplasia are: urgent urination to urinate and frequent urination both during the day (pollakiuria) and at night (nocturia), the terminal dripping (some drops of urine continue to come out), the sensation of a not complete emptying of the bladder.
Kidney damage can occur in cases of significant urinary retention.
How is the diagnosis performed?
The rectal exploration, that is the examination of the prostate performed through the anus, represents the first examination necessary to identify prostate hypertrophy. This control is recommended every year starting from 50 years of age, especially in patients who have had ascendants with a history of prostate cancer in the family.
Usually, instrumental examinations are associated such as: transrectal ultrasonography – to detect the size of the prostate – and, especially in the initial phases of urination difficulties, flowmetry – which measures the speed and strength of the urinary jet.
A venous test is accompanied by these checks to find out the value of the PSA, the specific prostate antigen, which, although not a specific tumor marker, may make it appropriate to request more in-depth examinations to exclude a possible tumor concomitant, and an examination of the urine.
Which drug therapies do you recommend?
There are no medical therapies that completely solve prostatic hypertrophy but therapies that improve the way the bladder is emptied, thus improving the above mentioned micturition disorders.
Usually the first beneficial effects are evident after a few weeks of therapy and it may take several months before obtaining the maximum result.
The drugs used are: hormonal inhibitors, they act by inactivating the enzymes that allow the transformation of testosterone into dihydrotestosterone (Dht), which, seems to participate in the process of enlarged prostate. The administration of these drugs reduces, over time, the volume of the gland but, it is not said, that completely solves the disorders of urination
Alpha blockers that relax the bladder neck and prostate muscle tone, improving urinary flow.
A separate chapter deserves the use of the bladder detrusor which avoids discomforts linked above all to urgency and frequency voiding. It is always important to remember that medications must be taken under strict medical supervision.
When is surgery necessary?
Surgery is performed either due to lack of improvement, after medical therapy, or due to complications arising. Performed, almost always in spinal anesthesia, it is performed transurethral (endoscopic prostate resection – TURP – with various methods).
Only the hypertrophic part of the gland is removed through the urethra, digging a sort of tunnel with the aim of widening the canal and facilitating urination. It is a minimally invasive operation that involves a hospital stay of a few days. In special cases, open surgery (ie with a supra-pubic cut) that has the same purpose and purpose as endoscopic resection, but which involves a longer post-operative period and with greater discomfort for the patient, may be indicated.
What do you suggest to patients for a correct prevention?
No direct correlations were found between food, diet and nutrition, moderate exercise and consumption of fruit and vegetables are recommended; limit fatty foods, red meats and alcoholic beverages. It is also necessary to avoid drinking too much water or other liquids in the evening, to reduce the need to urinate during the night, and always try to empty the bladder completely, trying to understand if the emptying is more satisfying from sitting to standing .
تضخم البروستاتا الحميد: الأسباب والأعراض والتشخيص والعلاج
يتكون تضخم البروستاتا الحميد ، والمعروف باسم البروستاتا المتضخمة ، من زيادة في حجم الغدة الواقعة مباشرة أسفل المثانة. البروستات لديه وظيفة إنتاج جزء من السائل المنوي. يحدث تضخم البروستاتا الحميد عادة بعد سن 50 عامًا وهو شائع جدًا في الفئة العمرية ما بين 60 و 80 عامًا: ويقدر أنه موجود في نصف ما يزيد عن 50 عامًا وفي ثلاثة أرباع الأشخاص الذين تزيد أعمارهم عن 80 عامًا. 40 ٪ من المرضى الذين يعانون من تضخم البروستاتا الحميد يحتاجون إلى العلاج.
ما هي أسباب هذا التوسيع؟
لسوء الحظ لا تزال الأسباب غير معروفة. بالنظر إلى ما يصاحب ذلك من تضخم البروستاتا مع تقدم العمر ، فإننا ندرس الفرضية القائلة بأن التغيير في التوازن الهرموني (إياس الذكور) وخاصة مستوى هرمون تستوستيرون ، هرمون الذكورة بامتياز ، يمكن أن تلعب دورا في وهذا يعني أن الهيكل الهرموني الجديد ، مع تباين نسبة الاندروجين / الاستروجين يمكن أن يفضي إلى تضخم غدة البروستاتا.
ما هي الأعراض التي تميز تضخم البروستاتا الحميد؟
لا يُظهر تضخم البروستاتا الحميد أعراضه الخاصة ، لكنه يظهر أعراضًا مرتبطة بصعوبة التبول: تضخم الغدة ، في الواقع ، جزء القناة الذي يربط المثانة بالخارج) الذي يعبرها يضيق العيار ويلزم المثانة إلى إرهاق لطرد البول المتراكم.
بمرور الوقت ، يمكن أن يضعف هذا الاضطراب ويجعل المثانة أقل أداءً ، والتي يمكن أن تصبح أكثر إصابة بسهولة ، وتنتج الحجارة وتجعل تصريف المثانة الكامل صعبًا حتى الاستبقاء الحاد.
الأعراض التي يمكن أن تنجم عن تضخم البروستاتا المهم هي: التبول العاجل للتبول والتبول المتكرر خلال النهار (pollakiuria) وفي الليل (بيلة ليلية) ، والتقطير الطرفي (تستمر بعض قطرات البول في الظهور) ، والإحساس ب لم يكتمل إفراغ المثانة.
يمكن أن يحدث تلف الكلى في حالات احتباس البول.
كيف يتم التشخيص؟
يمثل استكشاف المستقيم ، وهو فحص البروستاتا الذي يتم إجراؤه من خلال فتحة الشرج ، أول فحص ضروري لتحديد تضخم البروستاتا. يوصى باستخدام هذه السيطرة كل عام بدءًا من سن 50 عامًا ، خاصةً في المرضى الذين لديهم صعود لديهم تاريخ من سرطان البروستاتا في الأسرة.
عادةً ما ترتبط الفحوصات المفيدة مثل: الموجات فوق الصوتية عبر المستقيم – للكشف عن حجم البروستاتا – وخاصة في المراحل الأولية من صعوبات التبول ، قياس التدفق – والتي تقيس سرعة وقوة النفاثة البولية.
يرافق الاختبار الوريدي هذه الفحوصات لمعرفة قيمة PSA ، مستضد البروستاتا المحدد ، والذي ، على الرغم من أنه ليس محددًا للورم ، قد يجعل من المناسب طلب المزيد من الفحوصات المتعمقة لاستبعاد ما يصاحب ذلك من ورم ، وفحص البول.
ما هي العلاجات الدوائية التي تنصحني بها؟
لا توجد علاجات طبية تحل تمامًا تضخم البروستاتا ، ولكن هناك علاجات تعمل على تحسين طريقة إفراغ المثانة ، وبالتالي تحسين اضطرابات التبول المذكورة أعلاه.
عادةً ما تكون الآثار المفيدة الأولى واضحة بعد بضعة أسابيع من العلاج وقد تستغرق عدة أشهر قبل الحصول على النتيجة القصوى.
الأدوية المستخدمة هي: مثبطات الهرمونات ، وهي تعمل عن طريق تعطيل الإنزيمات التي تسمح بتحويل هرمون التستوستيرون إلى ثنائي هيدروتستوستيرون (Dht) ، والذي يبدو أنه يشارك في عملية تضخم البروستاتا. إن تناول هذه الأدوية يقلل مع مرور الوقت من حجم الغدة ، لكن لا يقال إنه يحل تماما اضطرابات التبول.
حاصرات ألفا التي تسترخي عنق المثانة ونغمة عضلات البروستاتا ، مما يحسن التدفق البولي.
الفصل المنفصل يستحق استخدام مثبط المثانة الذي يتجنب المضايقات المرتبطة قبل كل شيء بالإلحاح وإلغاء التردد. من المهم دائمًا تذكر أن الأدوية يجب أن تؤخذ تحت إشراف طبي صارم.
متى تكون الجراحة ضرورية؟
يتم إجراء الجراحة إما بسبب نقص التحسن أو بعد العلاج الطبي أو بسبب المضاعفات الناشئة. يتم إجراؤه دائمًا في التخدير الفقري ، ويتم إجراءه عبر الإحليل (استئصال البروستاتا بالمنظار – TURP – بطرق مختلفة).
تتم إزالة الجزء الضخامي فقط من الغدة من خلال مجرى البول ، وحفر نوع من النفق بهدف توسيع القناة وتسهيل التبول. إنها عملية جراحية طفيفة تتطلب الإقامة في المستشفى لبضعة أيام. في حالات خاصة ، قد يتم الإشارة إلى الجراحة المفتوحة (أي مع قطع فوق العانة) التي لها نفس الغرض والغرض من الاستئصال بالمنظار ، والتي تنطوي على فترة أطول بعد العملية الجراحية مع إزعاج أكبر للمريض.
ماذا تقترح للمرضى للوقاية الصحيحة؟
لم يتم العثور على ارتباطات مباشرة بين الغذاء والنظام الغذائي والتغذية ، ويوصى ممارسة معتدلة واستهلاك الفواكه والخضروات. الحد من الأطعمة الدهنية واللحوم الحمراء والمشروبات الكحولية. من الضروري أيضًا تجنب شرب الكثير من الماء أو السوائل الأخرى في المساء ، لتقليل الحاجة إلى التبول أثناء الليل ، ومحاولة دائمًا تفريغ المثانة تمامًا ، ومحاولة فهم ما إذا كان الإفراغ أكثر إرضاءًا من الجلوس إلى الوقوف .
Hipertrofia prostática benigna: causas, síntomas, diagnóstico, tratamiento
La hiperplasia prostática benigna, comúnmente conocida como próstata agrandada, consiste en un aumento en el volumen de la glándula ubicada inmediatamente debajo de la vejiga. La próstata tiene la función de producir una parte del líquido seminal. La hiperplasia prostática benigna generalmente ocurre después de los 50 años y es muy común en el grupo de edad entre 60 y 80 años: se estima que está presente en la mitad de los mayores de 50 años y en tres cuartos de los mayores de 80 años. El 40% de los pacientes con hipertrofia prostática benigna necesitan tratamiento.
¿Cuáles son las causas de esta ampliación?
Lamentablemente, las causas aún se desconocen. Dada la concomitancia de la hiperplasia prostática con la edad avanzada, estamos estudiando la hipótesis de que el cambio en el equilibrio hormonal (andropausia) y, en particular, el nivel de testosterona, la hormona masculina por excelencia, puede desempeñar un papel en lo que significa que la nueva estructura hormonal, con la variación de la proporción de andrógenos / estrógenos, podría favorecer el agrandamiento de la glándula prostática.
¿Qué síntomas caracterizan la hipertrofia prostática benigna?
La hipertrofia prostática benigna no muestra sus propios síntomas, pero se manifiesta con síntomas relacionados con la dificultad para orinar: la glándula agrandada, de hecho, comprime la parte del canal que conecta la vejiga con el exterior) que la cruza estrechando el calibre y obliga la vejiga se sobrecarga para expulsar la orina acumulada.
Con el tiempo, este trastorno puede debilitarse y reducir el rendimiento de la vejiga, lo que puede infectarse más fácilmente, producir cálculos y dificultar el drenaje completo de la vejiga hasta la retención aguda.
Los síntomas que pueden derivarse de una hiperplasia prostática importante son: micción urgente para orinar y micción frecuente tanto durante el día (polaquiuria) como por la noche (nocturia), el goteo terminal (algunas gotas de orina continúan saliendo), la sensación de un Vaciado no completo de la vejiga.
El daño renal puede ocurrir en casos de retención urinaria significativa.
¿Cómo se realiza el diagnóstico?
La exploración rectal, es decir, el examen de la próstata realizado a través del ano, representa el primer examen necesario para identificar la hipertrofia de la próstata. Este control se recomienda todos los años a partir de los 50 años de edad, especialmente en pacientes con antecedentes de cáncer de próstata en la familia.
Por lo general, los exámenes instrumentales se asocian como: ecografía transrectal, para detectar el tamaño de la próstata, y, especialmente en las fases iniciales de dificultades para orinar, flujometría, que mide la velocidad y la fuerza del chorro urinario.
Una prueba venosa se acompaña de estos controles para determinar el valor del PSA, el antígeno prostático específico, que, aunque no es un marcador tumoral específico, puede hacer que sea apropiado solicitar exámenes más profundos para excluir un posible tumor concomitante, y un examen de orina.
¿Qué terapias farmacológicas me recomiendan?
No existen terapias médicas que resuelvan por completo la hipertrofia prostática, sino terapias que mejoran la forma en que se vacía la vejiga, mejorando así los trastornos de micción mencionados anteriormente.
Por lo general, los primeros efectos beneficiosos son evidentes después de algunas semanas de terapia y pueden pasar varios meses antes de obtener el máximo resultado.
Los medicamentos utilizados son: inhibidores hormonales, actúan inactivando las enzimas que permiten la transformación de testosterona en dihidrotestosterona (Dht), que parece participar en el proceso de agrandamiento de la próstata. La administración de estos medicamentos reduce, con el tiempo, el volumen de la glándula, pero no se dice que resuelva por completo los trastornos de la micción.
Alfabloqueantes que relajan el cuello de la vejiga y el tono muscular de la próstata, mejorando el flujo urinario.
Un capítulo separado merece el uso del detrusor de vejiga que evita las molestias vinculadas sobre todo a la urgencia y la evacuación de frecuencias. Siempre es importante recordar que los medicamentos deben tomarse bajo estricta supervisión médica.
¿Cuándo es necesaria la cirugía?
La cirugía se realiza debido a la falta de mejoría, después de la terapia médica o debido a complicaciones que surgen. Realizado, casi siempre en anestesia espinal, se realiza transuretral (resección de próstata endoscópica – RTUP – con varios métodos).
Solo la parte hipertrófica de la glándula se extrae a través de la uretra, cavando una especie de túnel con el objetivo de ensanchar el canal y facilitar la micción. Es una operación mínimamente invasiva que implica una estadía en el hospital de unos pocos días. En casos especiales, puede estar indicada la cirugía abierta (es decir, con un corte suprapúbico) que tiene el mismo propósito y propósito que la resección endoscópica, pero que implica un período postoperatorio más largo y con una mayor incomodidad para el paciente.
¿Qué sugiere a los pacientes para una prevención correcta?
No se encontraron correlaciones directas entre alimentos, dieta y nutrición, se recomienda el ejercicio moderado y el consumo de frutas y verduras; Limite los alimentos grasos, las carnes rojas y las bebidas alcohólicas. También es necesario evitar beber demasiada agua u otros líquidos por la noche, para reducir la necesidad de orinar durante la noche y siempre tratar de vaciar la vejiga por completo, tratando de entender si el vaciado es más satisfactorio de estar sentado a estar de pie.